
Ventricular Tachycardia Versus Supraventricular Tachycardia with Aberrancy, Part 1
When studying wide complex tachycardias, students of electrocardiography always come across a discipline that is quite challenging at first: the differentiation between ventricular tachycardia and supraventricular tachycardia with aberrant conduction. The various criteria used to arrive at the correct electrocardiographic interpretation is a subject often revisited, albeit with much trepidation. I’ve seen a lot of trainees get grilled by their mentors and freeze. When I was a trainee, I struggled several times myself. Through time, it has become one of my favorite subjects to study and teach.
I decided to start a series of articles going back to the source material of the various criteria. While there are better summaries already published (I will link to three great summaries below), I think doing a ”deep dive” into the various criteria and putting some historical perspective might provide some insight for students who want to master the topic.
The Beginnings of the Morphology Criteria (Sandler, Swanick, and Marriott)
Before we take a close look at the classic study by Hein Wellens et al1, it should be acknowledged that they were not the first team to investigate the electrocardiographic differences of ventricular ectopy and aberrant conduction. Henry Marriot (of Marriott’s Practical Electrocardiography fame) laid a lot of groundwork on the subject, together with I. Alberto Sandler and Edward J. Swanick.2,4
(It is interesting that as I began doing the ”legwork” for this piece, I rediscovered the joys and peculiarities of reading old articles. There are some passages that don’t quite jive with today’s sensibilities. For example, Dr. Marriott’s article in Circulation with I. Alberto Sandler2 problematically started with the sentence:
To the untutored Western eye, the faces of oriental gentlemen are strikingly alike.
And they go on to compare this ”predicament” to the difficulty of distinguishing an ectopic ventricular beat and bundle branch block. Building on the metaphor, they further describe their methodology thus:
One promising approach to distinguish the Chinese from the Japanese from the Filipino would be to line up a number of each and empirically scan their features for generic differences.
Being Filipino, I found the opening paragraph troubling, to say the least. Now before you get out your pitchforks, I never got to know Drs. Sandler and Marriott personally so I won’t pass judgement. This was written in 1965, a time when the politics of race were — how shall I say it? — less enlightened.
But I digress. Let’s delve into the science.)
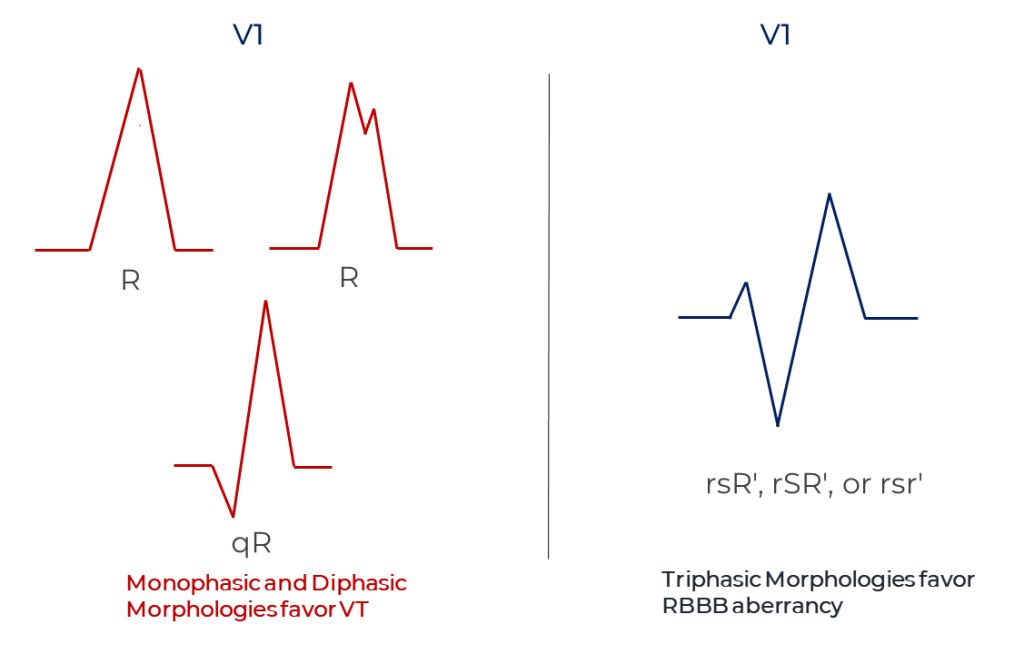
To start, Drs. Sandler and Marriott looked at ECG tracings with ventricular ectopic beats with right-bundle-branch-block-like morphology comparing them with ECG samples of fixed RBBB and RBBB aberrancy. They concentrated on the QRS morphology in lead V1 and concluded that a triphasic QRS complex — rsR’, rSR’, or rsr’ — favored aberrancy.2 In 1968, Marriott wrote a letter to the editor describing the observation that RBBB aberrancy usually had tripashic (qRs) complexes in lead V6 but ventricular ectopy had biphasic (rS) complexes. 3,12
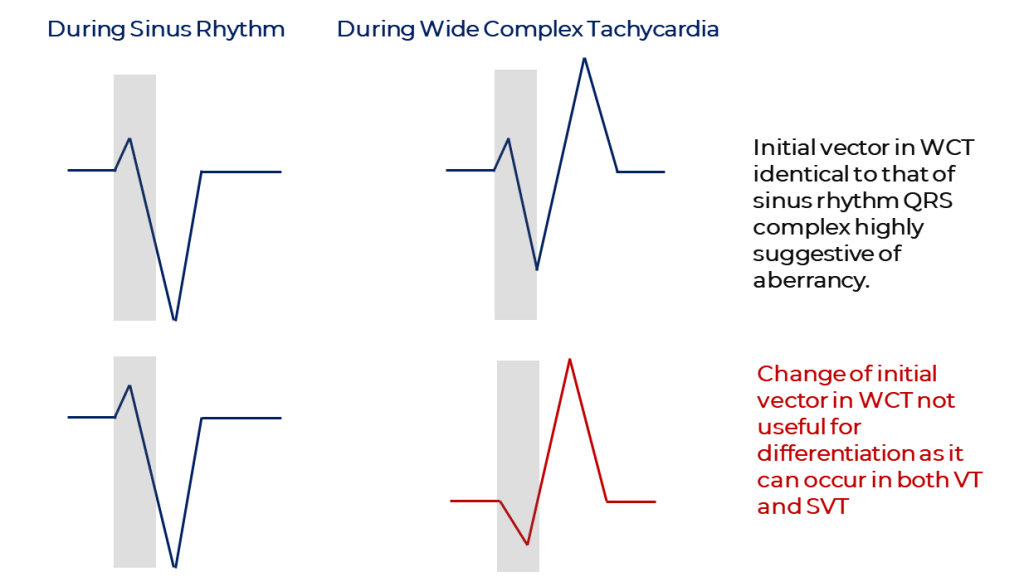
Another observation of Sandler and Marriott is that an initial vector identical to that in sinus rhythm is a strong evidence in favor of aberrant conduction.2 The corollary does not hold true though: a change in initial vector is not more consistent with ventricular tachycardia as it also occurs in aberrancy.2
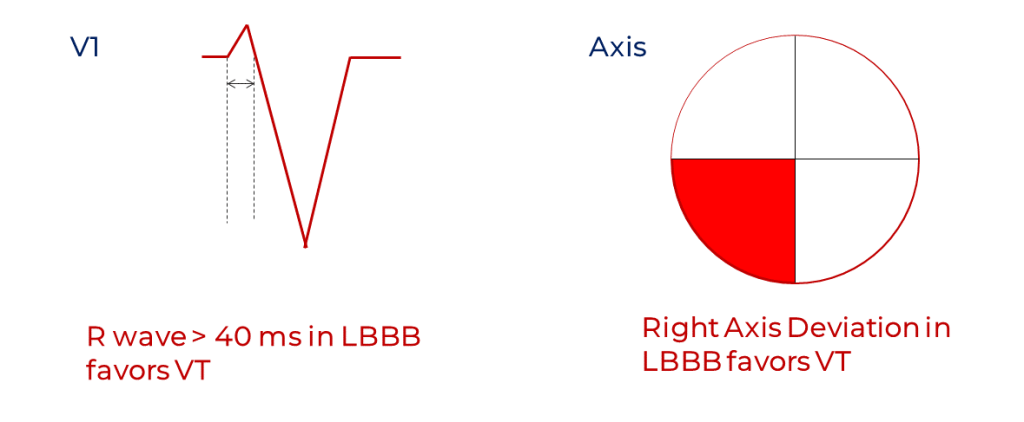
With Edward Swanick4, Marriott studied the morphologies of left bundle branch block and their findings were published in 1972. They looked at tracings of patients with known fixed left bundle branch block, tracings of induced right ventricular ectopic beats (thus of LBBB morphology) and samples of ventricular paced rhythm (pacing from the right ventricle, of course). They concluded that the following favored a diagnosis of ventricular ectopy: 1) a wide r wave (greater than 0.04 seconds) in V1, 2) a QS or rS complex deeper in lead V4 than in V1 and 3) right axis deviation.4
As a side note, the wide r in LBBB ventricular ectopic beats in V1 was also described in 1969 by Dr. Mauricio Rosenbaum:5
… this may be distinguished from the typical LBBB ECG pattern by the fact that the initial forces are directed pretty much anteriorly and are very slowly inscribed.
With his work with I. Alfonso Sandler2, Dr. Marriott laid the foundation of the RBBB morphology criteria. They started out mostly with conclusions about the QRS morphology in V1 but Dr. Wellens’ work would add observations for lead V6 later on1. Marriott’s collaboration with Edward Swanick4 was the groundwork for the LBBB morphology criteria on which both Hein Wellens1 and K. Elizabeth Kindwall10 would build on.
Dr. Marriott also discussed atrioventricular dissociation and precordial concordance in his summaries.12
The criteria of atrioventricular dissociation was widely known prior to Marriott’s time as it is something you can check during physical exam (i.e., presence of cannon a waves) but Marriott always stressed that it was not a reliable electrocardiographic parameter as it was not present in all ventricular tachycardia12. In other words, its presence highly suggests ventricular tachycardia but its absence doesn’t mean the diagnosis of aberrancy is more likely.
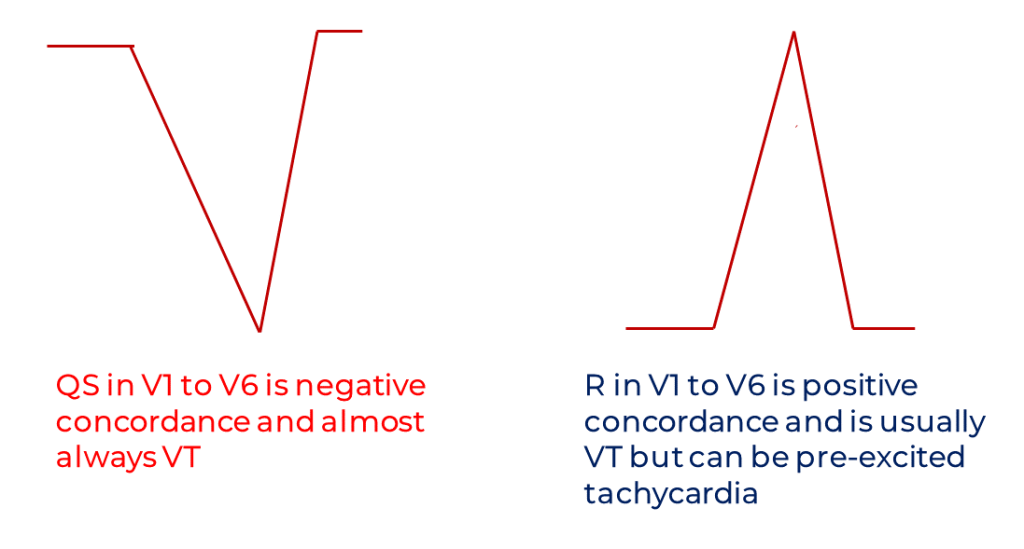
For precordial concordance, it should be clarified that Marriott (and most authors) define it as: 1) all positive QRS complexes / all monophasic R waves (positive concordance) or 2) all negative QRS complexes / all QS complexes (negative concordance)1, 8, 12, 13. Some have mistakenly defined it as all precordial leads mostly positive or all precordial leads mostly negative and this has caused some confusion. The presence of negative precordial lead concordance almost exclusively occurs in VT while positive concordance can still occur in pre-excited tachycardia.
I, like many others, have made the mistake of equating the absence of RS complexes in the Brugada criteria with concordance. But I have encountered examples of wide complex tachycardia that satisfy one and not the other. There was not one mention of concordance in the original Brugada algorithm paper13,14 so the two criteria are in fact different by definition and by underlying principle.8 (More about the Brugada criteria later on in the series.)
Cat and the Rabbit Ears
Everyone who has ever studied the right bundle branch block (RBBB) morphology criteria for VT has encountered the term “rabbit ears” or “bunny ears.” In one of his summaries, Dr. Marriott recounted that in 1968 it was a team of coronary care nurses that noticed that left ventricular ectopic beats tended to have two peaks in lead V112. They termed these peaks “rabbit ears” and the left rabbit ear was usually taller in ventricular ectopy (Rr’). Nurse Catherine “Cat” Gozensky, a protégé of Dr. Marriott’s, formally reported their observations in Heart Lung in 19747 but both Marriott and Gozensky described these very findings in earlier work.12
It is actually a misconception that the opposite configuration — that is, right rabbit ear taller than left rabbit ear or rR’ — strongly suggests RBBB aberrancy.7,8,9 This is probably because the classic triphasic rSR’ in V1 of RBBB aberrancy sort of fits the right-ear-taller description and has been used as an example by other authors. However, the term “rabbit ears” — in the original use of the term — was used to describe double-peaked R waves in monophasic (R) or biphasic (qR) complexes. True, left-ear-taller configuration (Rr’) strongly suggests ectopy, but right-ear-taller (rR’) configuration can be seen in either ectopy or aberrancy. With the right-ear-taller configuration in V1, one had to depend on the lead V6 criteria (a triphasic QRS and RS ratio > 1 in lead V6 are more in favor of an RBBB aberrancy). These findings are more evident when you look at subsequent studies and the consolidated morphology criteria.

The work of Cat Gozensky serves as a reminder for doctors, especially cardiologists, that nurses are not only integral in patient care but in the advancement of science and health education as well. Listen to your nurses, my friends!
Cat Gozensky recently passed away in February 20, 2020.6
The Wellens Criteria
Now on to the Wellens study.
Hein Wellens and his team were the first to use intracardiac electrograms to confirm the diagnosis of ventricular tachycardia or supraventricular tachycardia with aberrant conduction.1 They compared 70 electrophysiology study confirmed episodes of VT and 70 similarly confirmed recordings of SVT with aberrancy.
Their first observation was that ventricular tachycardia tended to be around 130 to 170 beats per minute in rate. They concluded also that a rate of 170 beats per minute and above in a wide complex tachycardia with RBBB morphology favored the diagnosis of supraventricular tachycardia (SVT) with aberrancy. These observations are no longer used in the modern criteria and Wellens himself in later articles concluded that the overlap of heart rates between SVT and VT made it a weak discriminator. (Anyone who has ever handled an implantable cardioverter defibrillator (ICD) knows that a lot of VTs go over 170 beats per minute.)
Their second observation is that atrioventricular dissociation during tachycardia favors VT. No surprise there.
Their next observation had something to do with QRS duration.
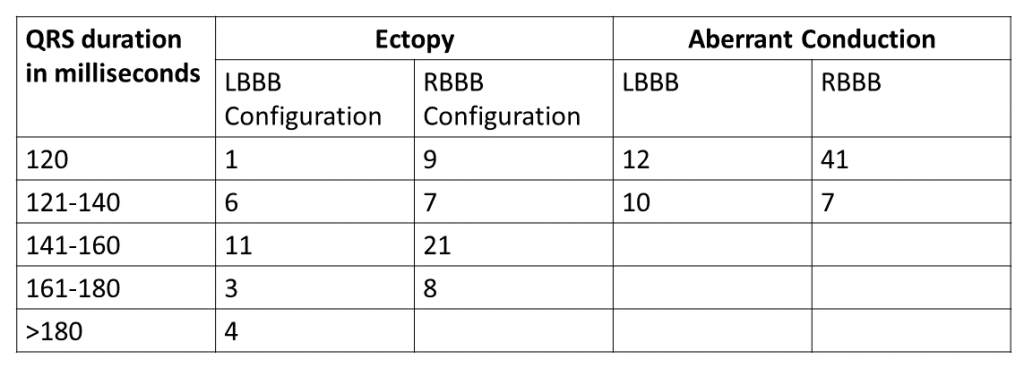
As you can see in Table 1, no episode of SVT with aberrancy had a QRS width of more than 140 milliseconds. Which means a QRS width more than 140 milliseconds favors VT. The wider the QRS, the higher the chance it’s VT. A QRS width of more than 160 beats per minute strongly suggests VT.
Now for the axis measurements.
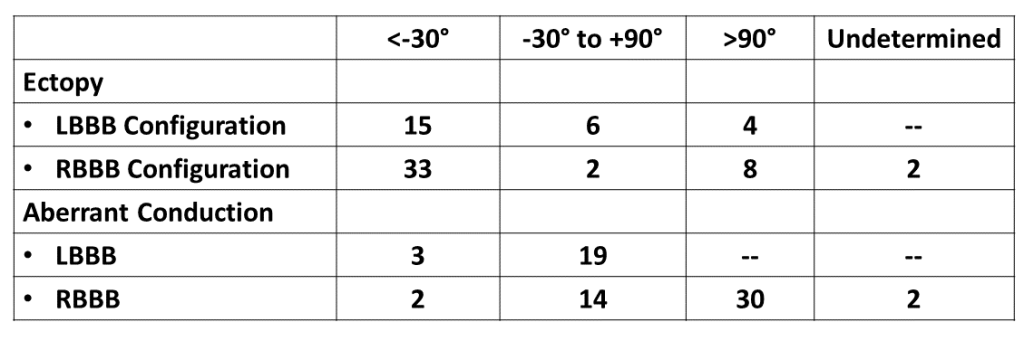
As you can see in Table 2, left axis deviation (<-30 degrees) favors the diagnosis of ventricular ectopy especially if with an RBBB morphology. No SVT with aberrant conduction with LBBB morphology had right axis deviation. So this is actually consistent with the observations of Swanick and Marriott that right axis deviation in LBBB morphology suggests VT. (Interestingly, Wellens et al only pointed out the left axis deviation criteria and generalized the observation to both types of BBB.)
Now to the juicy part of the study, the morphology observations in RBBB. Let’s start with V1 morphology in RBBB.
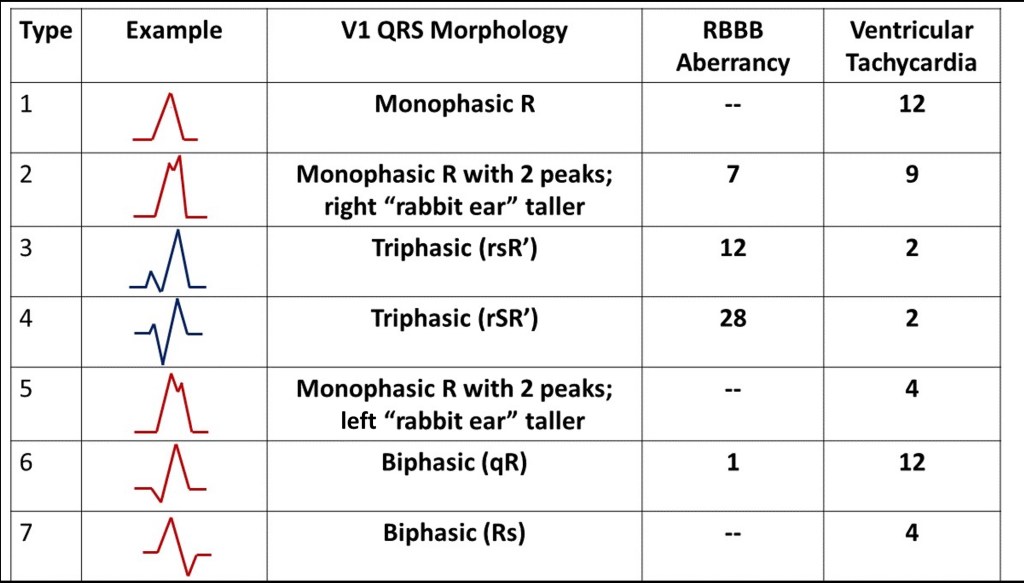
Let’s clarify a few things first. Marriott and Wellens did not use the same definitions of ”triphasic” in their respective papers. In Table 3, I use Marriott’s terms2. Marriott called Type 2 and 5 monophasic (albeit with two peaks or a notch) while Wellens called them triphasic1. I will stick to the convention that a wave is not a wave unless it crosses the baseline. So Type 2 and 5 are not ”triphasic” in the sense that they are not rsR’ or rSR’ but rR’ and Rr’. Wellens called Type 3 and 4 “classic triphasic” QRS complexes1.
The findings are pretty clear when you look at Table 3. Type 3 and 4 complexes (triphasic complexes) are more likely to be present in SVT with aberrancy. Type 1, 6, and 7 complexes (monophasic and biphasic complexes) almost always occur in VT. Type 2 complexes (monophasic with right rabbit ear taller) can be present in both SVT with aberrancy and VT. In agreement with the observations of Marriott and Gozensky, Type 5 complexes (monophasic with left rabbit ear taller) only occurs in VT. The presence of Type 5 complexes in V1 is also known as Marriott’s sign.
Let’s go to V6 then.
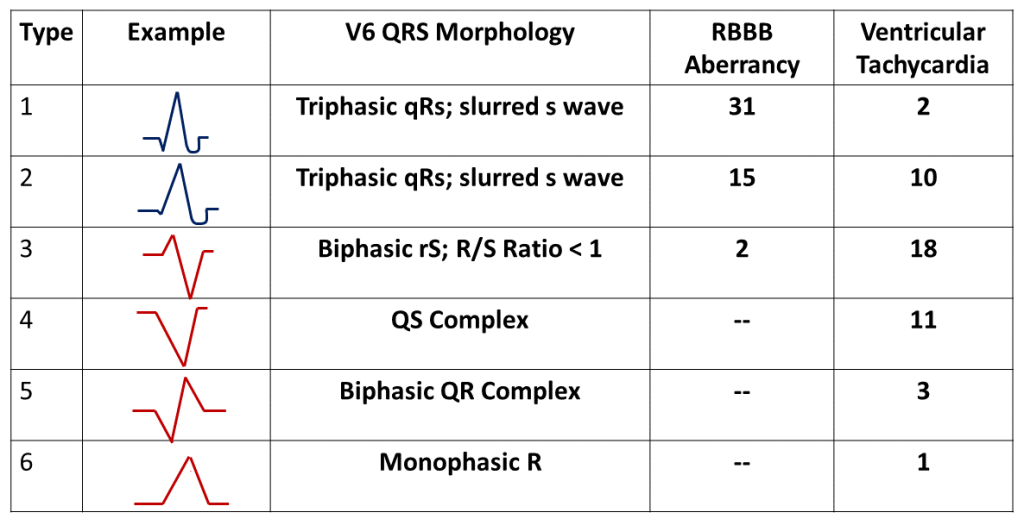
The triphasic qRs configurations (Type 1 and 2) are clearly typical RBBB findings in V6 and not surprisingly favor the diagnosis of SVT with aberrant conduction. Types 3 and 4 are biphasic rS and monophasic QS, configurations that both satisfy the description of R/S Ratio < 1. Type 5 and 6 are again biphasic and monophasic (QR and R) and only occur in VT.
Suprisingly, the Wellens study did not see any differences in V1 morphology in LBBB. So let’s take a look at what they saw for LBBB morphology in V6.
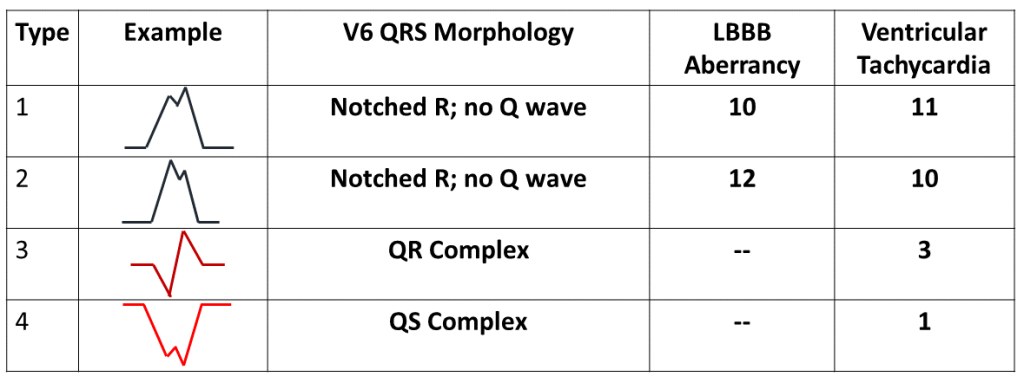
Type 3 and 4 morphologies (QR and QS) are only seen in ventricular tachycardia while Type 1 and 2 are seen in both LBBB aberrancy and VT. Since the loss of the septal Q wave is part of typical left bundle branch block, Wellens’ team concluded that the presence of any Q wave in V6 favors the diagnosis of VT1.
Lastly, there were two ventricular tachycardia patients in this study noted to have precordial concordance.
To recap, the observations of Wellens in this study are as follows:1
- Atrioventricular dissociation in a wide complex tachycardia favors ventricular tachycardia.
- A QRS width of more than 140 milliseconds suggests ventricular tachycardia.
- Left axis deviation suggests ventricular tachycardia.
- Mono- or biphasic QRS complexes in lead V1 in RBBB-like morphology tachycardia favor VT. “Classic triphasic” or rSR’ or rsR’ complexes favor the diagnosis of SVT with aberrancy. Double peaked R with left rabbit ear taller is consistent with VT. Double peaked R but with right rabbit ear taller (rR’) can either be aberrancy or VT.
- An R/S ratio < 1 in lead V6 in a wide complex tachycardia with RBBB-like morphology is consistent with VT.
- The presence of a Q wave in lead V6 in a wide complex tachycardia with LBBB-like morphology is consistent with VT.
- Precordial concordance (“entirely upright or entirely inverted complexes”) is consistent with VT.
Wellens et al did not state any significant findings for lead V1 in LBBB.1 So aside from Swanick and Marriott’s work, what is the V1 morphology criteria for LBBB based on? Enter K. Elizabeth Kindwall and Mark E. Josephson.
Final Pieces of the Puzzle? The Kindwall Criteria for LBBB and the Akhtar Study
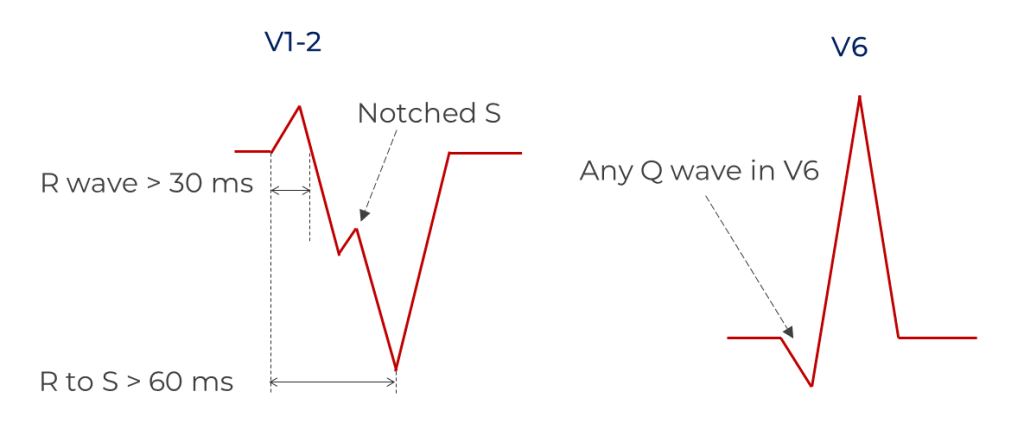
Noting the paucity of data on LBBB morphology criteria, the team of K. Elizabeth Kindwall compared the 12 lead electrocardiograms of 118 patients with LBBB morphology wide complex tachycardia.10 They confirmed the diagnosis of VT or SVT with aberrancy via an electrophysiologic study and looked at four criteria: 1) R wave > 30 ms in duration in V1 or V2, 2) Any Q wave in V6, 3) R to nadir of S wave >60 ms in V1 or V2 and 4) notched downstroke S wave in V1 or V2. These criteria were likely based on the observations of various people including Swanick (wide R in V1), Marriott, Wellens and Mark E. Josephson (the notched S wave, also known as the Josephson Sign).
They found that each criterion taken alone had high predictive accuracy and specificity for ventricular tachycardia but relatively low sensitivity. However, these had a higher sensitivity as combined criteria. The group also concluded that left axis deviation was not a useful distinguishing feature in LBBB morphology wide QRS tachycardia, as it occurs with similar frequency in both VT and SVT with aberrancy.
Dr. Masood Akhtar and his team published a paper in the same year and their QRS duration and frontal axis observations are also often quoted alongside the “Classical” Criteria.11 Their study looked at the ECGs of 150 consecutive patients with wide complex tachycardia. Electrocardiographic confirmation was required in this study as well. It wasn’t clear how they defined monophasic, biphasic and triphasic QRS configurations as they did not show examples, but their data on morphological criteria (Sandler and Marriott’s RBBB criteria2 and R to nadir of S > 70 ms in LBBB) were disappointing. They found however that following ECG criteria favored VT: atrioventricular dissociation, positive concordance, extreme axis deviation (“no-man’s-land” as described by Marriott in 197212), QRS duration of > 140 ms in RBBB, QRS duration > 160 ms in LBBB and morphology during tachycardia different from baseline pre-existing bundle branch block.11
Bringing It All Together: The Classical Criteria
The Classical Criteria is occasionally referred to as the Classical Wellens Criteria or the Classical Morphology Criteria. However, these criteria do not exclusively involve just Wellens’ work and QRS complex morphology.
To remember the Classical Criteria, take note of the following:
- AV dissociation. Atrioventricular dissociation favors ventricular tachycardia. The presence of capture and fusion beats are proof of atrioventricular dissociation but are usually found in slower VTs.
- QRS duration. A QRS width of more than 140 milliseconds suggests ventricular tachycardia in RBBB. A QRS duration > 160 milliseconds suggests VT in LBBB.
- Frontal axis deviation. Left axis deviation suggests ventricular tachycardia in RBBB morphology tachycardia. Right axis deviation suggests ventricular tachycardia in LBBB morphology tachycardia. Extreme axis deviation strongly points to VT.
- Concordance. Precordial lead concordance (entirely positive or entirely negative complexes) is consistent with VT. Negative concordance is almost always VT while positive concordance could still be pre-excited tachycardia.
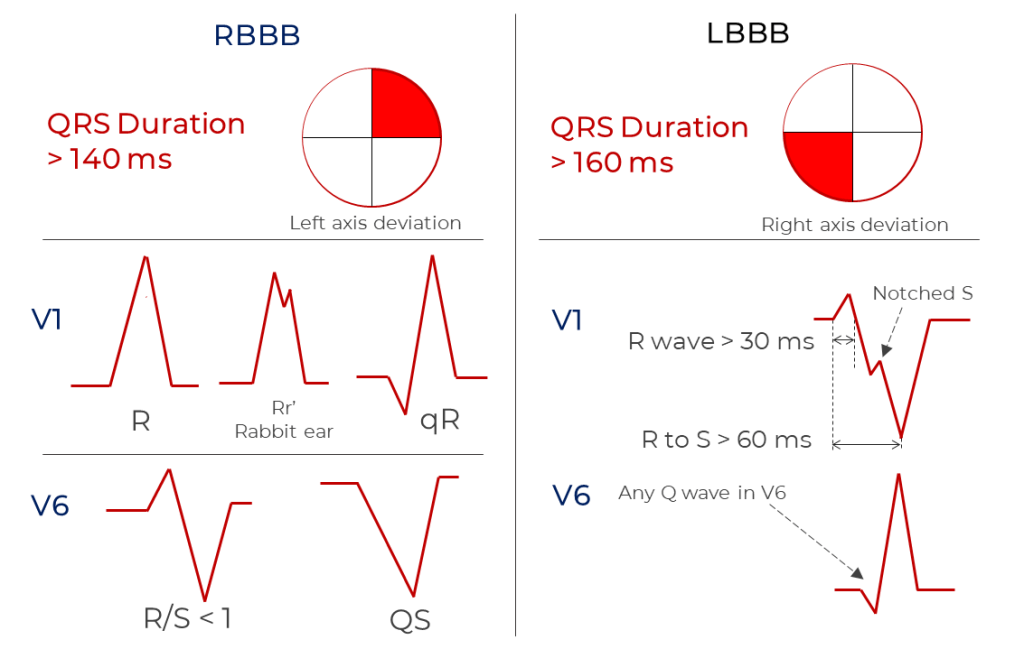
- Morphology Criteria. Atypical right bundle or atypical left bundle branch block morphology in V1 and V6 favors VT (see figure).
There you have it. As you can see, the “Classical Criteria” involve texts from the 1960s up to the late 1980s. The next innovation will come in the 1990s, the step-wise algorithmic approach to wide complex tachycardia differentiation as pioneered by Josep and Pedro Brugada.14
Footnotes
- H J Wellens, F W Bär, K I Lie. The Value of the Electrocardiogram in the Differential Diagnosis of a Tachycardia With a Widened QRS Complex. Am J Med. 1978 Jan;64(1):27-33. doi: 10.1016/0002-9343(78)90176-6. [Link]
- Sandler, IA and Marriot, HJ. The differential morphology of anomalous ventricular complexes of RBBB type in lead V1: Ventricular Ectopy Versus Aberration. Circulation. 1965 Apr;31:551-6. doi: 10.1161/01.cir.31.4.551. [Link]
- Marriott HJL, LaCamera F: Diagnosis of arrhythmia (letter to editor). JAMA. 1968. 203:527-528.
- E J Swanick, F LaCamera Jr, H J Marriott. Morphologic Features of Right Ventricular Ectopic Beats. Am J Cardiol. 1972 Dec;30(8):888-91. doi: 10.1016/0002-9149(72)90015-x. [Link]
- Rosenbaum, M. Classification of ventricular extrasystoles to form. J Electrocardiol. 1969 Jul;2(3):289-97. doi: 10.1016/s0022-0736(69)80091-9. [Link]
- Obituary: Catherine Bernice “Cat” (Gemmel) Volkmann. URL: https://www.legacy.com/obituaries/theledger/obituary.aspx?n=catherine-bernice-volkmann-cat-gemmell&pid=195589637&fhid=6779. [Link]
- Gozensky C and Thorne D. Rabbit Ears: An Aid in Distinguishing Ventricular Ectopy From Aberration. Heart Lung. Jul-Aug 1974;3(4):634-6. [Link]
- Vereckei A. Current algorithms for the diagnosis of wide QRS complex tachycardias. Curr Cardiol Rev. 2014;10(3):262‐276. doi:10.2174/1573403×10666140514103309. [Link]
- Jerry W. Jones. “Rabbit Ears” and Right Bundle Branch Block. Dr. Jones’ ECG Blog. March 8, 2018. URL: https://medicusofhouston.com/rabbit-ears-and-right-bundle-branch-block/ [Link]
- KE Kindwall, J Brown, ME Josephson. Electrocardiographic Criteria for Ventricular Tachycardia in Wide Complex Left Bundle Branch Block Morphology Tachycardias. Am J Cardiol. 1988 Jun 1;61(15):1279-83. doi: 10.1016/0002-9149(88)91169-1. [Link]
- Akhtar, Masood; Shenasa, Mohammad; Jazayeri Mohammad; Jose, Caceres; Tchou, Patrick J. Wide QRS Complex Tachycardia: Reappraisal of a Common Clinical Problem. Ann Intern Med. 1988 Dec 1;109(11):905-12. doi: 10.7326/0003-4819-109-11-905. [Link]
- HL Marriott. Differential Diagnosis of Supraventricular and Ventricular Tachycardia. Cardiology. 1990; 70: 209-220. [Link]
- Jerry W. Jones. Precordial Concordance in VT. Dr. Jones’ ECG Blog. July 8, 2019. URL: https://medicusofhouston.com/precordial-concordance-in-vt/ [Link]
- Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation. 1991;83:1649–59. [Link]
Great Summaries
Vereckei A. Current algorithms for the diagnosis of wide QRS complex tachycardias. Curr Cardiol Rev. 2014;10(3):262‐276. doi:10.2174/1573403×10666140514103309. [Link] This is an excellent review by Andras Vereckei and I like to call it the Vereckei Summation. For more advanced readers.
John B. Garner and John M. Miller. Wide Complex Tachycardia – Ventricular Tachycardia Or Not Ventricular Tachycardia, That Remains The Question. Arrhythmia & Electrophysiology Review 2013;2(1):23-9. DOI: https://doi.org/10.15420/aer.2013.2.1.23. [Link]
Anthony H. Kashou, Peter A. Noseworthy, Christopher V. DeSimone, Abhishek J. Deshmukh, Samuel J. Asirvatham, and Adam M. May. Wide Complex Tachycardia Differentiation: A Reappraisal of the State‐of‐the‐Art. J Am Heart Assoc: e016598.
https://doi.org/10.1161/JAHA.120.016598. [Link]

Leave a comment